WWII battle scene. A medic comes upon a wounded soldier and gives him IM morphine When IV fluids are administered to combat the fluid loss, the soldier develops respiratory distress and dies.
WHY? The patient was in shock, there is not much blood in the tissues where the morphine was injected, once volume is replenished, the large opiate dose is available and hits the brain hard.
Absorption:
the area of the absorbing surface to which a drug is exposed (in this case circulating blood in the muscle) is one of the more important determinants of the rate of blood absorption.
The brain concentration of drug follows the concentration of the plasma
Morphine
is a weak organic base with pKa = 9; plasma pH = 7.4, therefore morphine is ionized in plasma
Pavlov gave one dog IV morphine, but found both dogs became intoxicated; morphine localized in the gut and induces vomiting, so it was ingested by the other dog (respiratory center Þ toxicity)
Distribution
Blood Flow:
Heart, liver, brain, and other well perfused organs receive most of the drug during the first few minutes of absorption. Delivery of a drug to muscle, most viscera, skin, and fat is slower and these tissues may take hours to establish a steady-state.
Superimposed on the pattern of distribution of blood flow are:
Membranes
: diffusion into the interstitium occurs rapidly due to the highly permeable nature of capillary endothelial membranes. The Blood Brain Barrier (BBB) limits what can get into the brain.
Drugs accumulate in tissues
due to pH gradients, binding to intracellular constituents, or partitioning into lipid. WOA as pH ß more non-ionized forms // WOB as pH ß more ionized
WOA’s accumulate in tissues with elevated pH; WOB’s, in tissues with lower pH
Drugs accumulated in tissues may serve as reservoirs that prolong drug action.
Drugs binding to proteins
: Albumin Þ WOA’s // a 1-acid glycoprotein Þ WOB’s
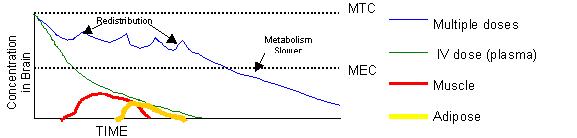
Thiopental A
single IV dose gives a rapid onset of anesthesia, but its effect lasts less than a ½ hour. However multiple doses of Thiopental have longer action and take longer to recover from.
Thiopental’s time is the therapeutic range is relatively short; goes to brain because it is a WOA (pKa=7.5), so equal ratio of ionized and unionized
Once in the plasma the onset of drug action is rapid (because given IV and going to brain)
Thiopental dissipates more slowly when given in multiple doses because a steady-state is reached; it accumulates in the fat (low blood distribution), so it takes a while to dissipate.
As one administers more drug, the drug begins to accumulate in the muscle and adipose tissues (muscle capacity is larger, but it takes longer to distribute there). These tissues serve as reservoirs. An equilibrium is established between the reservoirs and plasma.
The lipid soluble form is re-absorbed by the kidney so the lipid soluble form has to undergo a change to become more water soluble so as to be excretable.
Single dose
Þ redistribution of drug between tissues lowers drug concentration
Multiple dose
Þ metabolism to lower drug concentration; metabolism is slower than redistribution
The Volume of Distribution
Dose (mg)
µ concplasma (mg/L) – need a constant to convert mg to mg/L Þ that constant is THE VOLUME OF DISTRIBUTION (it is not a real volume)
VD = dose/conc; The VD relates the amount of drug in the body to the concentration of drug in the plasma.
The VD may vary depending on pKa, binding to plasma proteins, the lipid:water coef, binding to tissues,etc
Example:
Digoxin is used to treat CHF
Fo
» 1; Dose = 0.3 mg; Concentration = 0.8 ng/mL
VD = (0.3mg) / (0.8 x 10-6 mg/mL) = 375 Liters
Digoxin is not in the plasma. Digoxin is bound in tissues. Sequestration can help (e.g. Chloroquine is sequestered in the liver, a feature that is used when treating for amebiasis). Sequestration can harm (e.g. Gentamycin builds up in the hair cells of the ear and can lead to hearing loss.)