"62% of Americans believe you need to have one bowel movement per day for good health" --- NOT TRUE!!
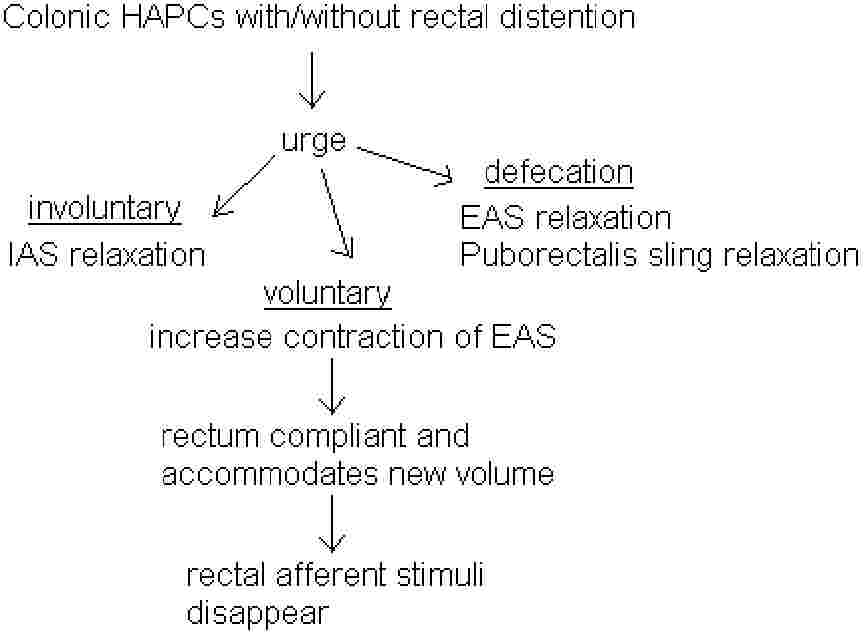
Colonic Contractile Patterns: phasic contraction, tonic contraction, high amplitude propagating contractions (HAPC) like migrating myoelectric complex.
Basic Functions
Ascending Colon – Mixing and water absorption
Transverse and Descending Colon – Propulsion
Sigmoid Colon and Rectum – Reservoir
Anal Sphincteric Mechanism of Continence
Internal Anal Sphincter (IAS) – composed of smooth muscle maintained in a state of near maximal contraction at all times. Resting electrical activity consists of slow sinusoidal waves (like GI smooth muscle), with contraction of myogenic origin. Major reflex response is relaxation.
External Anal Sphincter
(EAS) – composed of skeletal muscle maintained in a state of minimal contraction, varying with posture and alterations of abdominal pressure. Resting electrical activity consists of infrequent APs (rapid spikes) characteristic of striated muscle. Contraction is neurogenic. Electrical activity persists during sleep. EAS does NOT degenerate, even when denervated.
Retrosphincteric Reflexes
IAS – Relaxation only induced by rectal distention, and probably mediated via myenteric plexus (IAS reflex persists after denervation). Electrical activity is inhibited during relaxation.
EAS – Relaxation induced by rectal distention, voluntary effort, postural change, perianal scratch,
Ý abdominal pressure, and anal dilatation. Afferent impulses travel centrally in dorsal fiber of S2. Efferent limb is via pudental nerves which exhibit a crossover of motor fibers.
Sensory Innervation of the Anorectal Area
Rectum is only sensitive to stretch stimuli, but (anorectal area) can differentiate between gas, liquid, and solid states of matter. (amazing!)
Distal anal canal specialized nerve endings:
Meissner’s corpuscles – sensitive to touch
Krause bulbs – sensitive to cold
Golgi-Mazonni bodies – sensitive to pressure
Genital corpuscles – sensitive to friction
Pathophysiology of Anorectal Disorders
Hirschsprung’s Disease
Absence of parasympathetic ganglion cells from the submucosal and myenteric plexuses in the distal colon.
Results in functional colonic obstruction:
(1) Failure of propulsive forces in affected segment.
(2) IAS contracts instead of relaxing after rectal distention.
(3) Sympathetic hyperactivity and
ß serotonergic nerve activity leads to state of constant contraction.
Etiology
: arrest of migration of neural crest cells from the notocord during development, and/or Ý destruction of ganglion cells by temporal bowel ischemia in-utero.
Presentation
: Variable. Delayed passage of meconium, vomiting, abdominal distention, sudden enterocolitis (diarrhea, prostration, fever), only diarrhea, constipation. Can be mistaken for functional bowel disease in older kids.
Treatment
: Medical include resuscitation and nutritional support, surgical include resection and low anastomosis at age 1-2 years. Colostomy, rectal biopsy in newborn period.
Sphincter Incontinence
Factors disturbing normal control
: Chronic functional megacolon in children, CNS or spinal cord injuries, disturbances/loss afferent sensory component of rectosphincteric reflexes, scleroderma (impairs smooth muscle) or polymyositis (impair striated muscles), direct muscle damage (disease/trauma), aging.
Major reason why women get incontinence, even decades after birth, is child birth. Muscles get ripped/damaged.
Treatment
: Biofeedback treatment includes having patient see their own attempts during a monometry test. May reinstitute automatic reflex contration of EAS.
Anal Fissures
Abnormal sphincter spasm occruing after the anus is dilated (extrusion of stool, balloon distention, etc). Medical or surgical treatment is associated with disapperance of this abnormal sphincter reflex.
Internal Hemorrhoids
Probably caused by higher than normal anal pressures.
Constipation
definition, 2 or more of the following for at least 3 months:
(1) Two or fewer bowel movements per week.
(2) Stool weight < 35 g; Straining >25%.
(3) Hard and lumpy stools >25%.
(4) Sensation of incompleteness >25%.
Constipation in Childhood
– #1 reason kids don’t control bowels is constipation!!!
Congenital
Hirschsprung’s Disease
Anorectal Malformations
Cystic Fibrosis
Acquired
Functional Fecal Retention (encopresis)
Colonic Motility Patterns Leading to Constipation
Functional outlet obstruction.
Increase in segmental phasic contractions.
Decrease in Phasic contractions (Colonic Intertia).