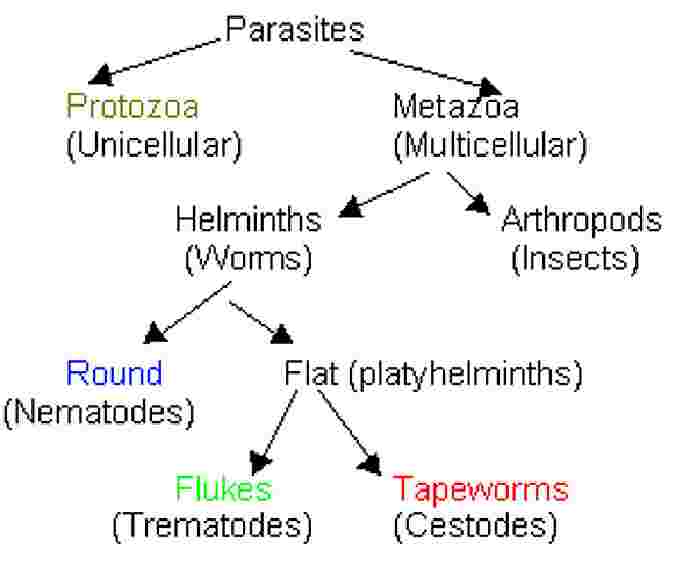
The flatworms are split into flukes (Trematodes) or tapeworms (Cestodes).
Flukes live in tissues, tapeworms live in the gut.
Protozoan Parasites
Giardia Lamblia
– a flagellate protozoan, primitive eukaryote (no mito, no peroxisomes, primitive ER and Golgi), a common cause of waterborne diarrheal outbreaks in the U.S.. Water borne, fecal-oral, and food borne.
Life cycle
– the Cyst is ingested, passes into small intestine where it excysts releasing the Trophozoite. The replicative phase, the Trophozoite, stays in close association with the mucosa, makes and releases cysts into the gut lumen Þ stool. The cyst has GalNAc as a major sugar on its wall. Chlorination does not kill the cysts.
Mechanism
– not known for sure, but immunological reaction to the parasite appears to interfere with CHO absorption causing diarrhea and flatulence. Common symptoms are diarrhea, abdominal bloating and pain, as well as weight loss.
Diagnosis
– microscopy of stool (trophozoites in diarrhea, cysts in formed stool), H and E of biopsy or immunological markers. Incubation period of 1-2 weeks, self limiting in ~6 weeks (in immunocompetent).
Treatment
– Nitroimidazoles.
Entamoeba histolytica
– with its morphologically similar but non-pathogenic cousin E. dispar, infect 10% of the world. (3rd leading cause of death due to parasites in the world). Large outbreaks are uncommon.
Life cycle
– cysts ingested, excyst in distal ileum, trophozoites live in the colon and make cysts which get excreted in stool.
Mechanism
–majority of people are asymptomatic. E. histolytica causes intestinal (dysentery) or non-intestinal disease (liver abscess). When non-intestinal patient’s have little abdominal pain but have small colonic lesions on colonscopy.
Pathogenesis of Invasive Amoebic Disease
(1) barrier breakdown
(2) adherence (via Gal/GalNAc lectin)
(3) injury/lysis of targets cells
(4) phagacytosis
(5) translocation (has to get to the liver to form abscesses)
extra intestinal manifestations include hepatic abscesses, pericardial and pleuropulmonary problems, also GU problems.
Diagnosis
– can visualize the amoeba that has eaten a RBC in fresh stool samples. Liver abscesses are seen on ultrasound.
Treatment –
Nitroimidazoles to treat invasive stage, other drugs (Paromomycin) needed to treat the luminal stage.
Once adhered, E. histolytica delivers a "lethal hit" to the target cell. The parasite then phagacytizes the dead cell and recruits an immune response (furthering damage)
Cryptosporidium parvum
– prevalent, infects ruminants (cattle), most frequent waterborne diarrheal outbreak.
Life cycle
– Complex. (paraphrased from syllabus)
Infection is acquired by the ingestion of oocysts. Excystation, in the small intestine, results in a sporozoite that lives in the INTRAMEMBRANOUS SPACE between the opposing layers in the lipid bilayer. The sporozoite differentiates into a trophozoite, undergoes a complex cycle of growth and differentiation (merogony) to become type I meronts with 6 to 8 merozoites. When type I meronts rupture the released merozoites can attach to nearby epithelial cells. Their development can result either in type I or type II meronts, which produce 4 merozoites , invade host cells and become micro (male) or macro (female) gamonts. Microgamonts multiply resulting in up to 16 micragametes, which fuse with mature macrogametes resulting in a zygote. This develops by sporogony into thick wall oocysts (80%) which are excreted in feces or thin walled oocysts (20%) which can excyst in the host and reinfect cells.
Mechanism
– not well understood, morphologic and functional alterations due to infection load as well as immune response are probably the mechanisms resulting in altered salt and water transport and malabsorption of CHO and nutrients. Symptoms include; profuse watery diarrhea, malabsorption and weight loss, abdominal pain, flatulence, N/V, but no fever.
Self limiting in < 3 weeks in the immunocompetant // serious disease in immunocompromised (AIDS).
Diagnosis
– acid fast stain of stools shows red oocysts. Immunologic tests or serologic tests available too.
Treatment
– Supportive care is indicated. Most drugs are suboptimal. Paromomycin is the most promising agent.
Worms
Ascaris lumbricoides
– the largest nematode infecting humans.
Life cycle
– ingestion of eggs (ova)Þ larvae in small intestine Þ liver Þ lungs Þ coughed up and swallowed Þ intestine
Adult worms live in the intestine producing eggs that exit in the stool. (lifespan = 6mo-1yr)
Mechanism
– a heavy worm load can cause intestinal obstruction (common in the developing world) and undernutrition. Disease with a light worm load may be due to obstruction of the pancreatic or bile ducts (biliary colic and/or pancreatitis).
Diagnosis
– eggs in stool
Treatment
– mebendazole, pyrantel pamoate, albendazole.
Strongyloides stercoralis
– common infection in developing nations (and Kentucky). Can persist for years because its full life cycle can be completed in humans.
Life cycle
– adult female lays eggs in the mucosa. These eggs develop into Rhaditiform larvae (thick) which pass out in the stool, or into Filiform larvae (thin) which are capable of penetrating intact skin. The filiform larvae travel to lung capillaries via blood vessels, burrow through alveoli, coughed up and swallowed back to the small intestine where they become adults and lay their own eggs. Transient skin and lung symptoms occur during migration. Glucocorticoid treatment can increase the amount of filiform larvae produced.
Diagnosis
– need a great deal of stool to see Rhaditiform larvae. Sometimes one can see cutaneous marks left from filiform larvae migration. Serologic and molecular markers are helpful but currently are not readily available
Treatment
– Thiabendazole is recommended.
Taenia solium
– pork tapeworm, 20-30 meters long! Have a head (scolex) which has four suckers and hooklets. Also the body is made up of segments (proglottids), each segment having male and female parts.
Life cycle
– Adult stage is in the definitive host, larval stage is in the tissues of another species. Adult worms live in the small intestine. Intact proglottids or the released eggs are passed out in the stool. Larvae are released by the eggs when consumed by the intermediate host (pig). The larvae travel to and encyst in the skeletal muscle. Humans acquire the infection by eating undercooked pork and the encysted larvae develop into adults in the human intestine.
Mechanism
– infection is usually asymptomatic. If eggs are ingested Cysticercosis develops where larvae encyst in the human’s brain. Neurologic symptoms usually predominate.
Diagnosis
– diagnosis is by recognizing the proglottid or eggs is the stool. Cysticercosis is recognized by imaging studies
Treatment
– Praziquantel to treat intestinal infection. Surgery in addition to drugs may be necessary in Cysticercosis.