problems with [HCO3-] are metabolic acid-base disorders
problems with PCO2 are respiratory acid-base disorders
CO2 which is a potential acid in the body fluids (H2CO3) is termed = volatile acid
Any other acids derived from the diet are termed = nonvolatile acids
Overview
Approximately 70 mEq/day of nonvolatile acids are produced. Nonvolatile acids are buffered in the ECF as Na+ salts. To maintain acid-base balance the kidney must excrete these Na+ salts and replenish the HCO3- lost by the buffering process.
Example: H2SO4 + 2 NaHCO3
Þ Na2SO4 + 2CO2 + 2H2O
To maintain acid-base balance, net acid excretion must equal nonvolatile acid production, all in while preventing the loss of HCO3- in the urine. This is important because approximately 4,320 mEq/day of HCO3- are filtered.
Both the reabsorption of filtered HCO3- and the excretion of acid are accomplished through the process of H+ secretion by the nephrons. Thus in a single day the nephrons must secrete approximately 4,390 mEq of H+ into the tubular fluid. Most of the H+ does not leave the body in the urine but serves to reabsorb the filtered load of HCO3-. Only 70 mEq are excreted. As a result of this acid excretion, the urine is normally acidic. (note how the numbers add up perfectly).
Why not just reverse the reaction to excrete the nonvolatile acid and replenish HCO3- ???
Reversing the reaction would yield a urine that has a pH=1.0. The minimum urine pH is only 4.0 to 4.5. Consequently, the kidneys cannot excrete the free acids but must excrete their Na+ salts, while at the same time excreting the H+ with other urinary buffers. The two major urinary buffers are ammonia (NH3/NH4+) and phosphate (HPO42-/H2PO4-).
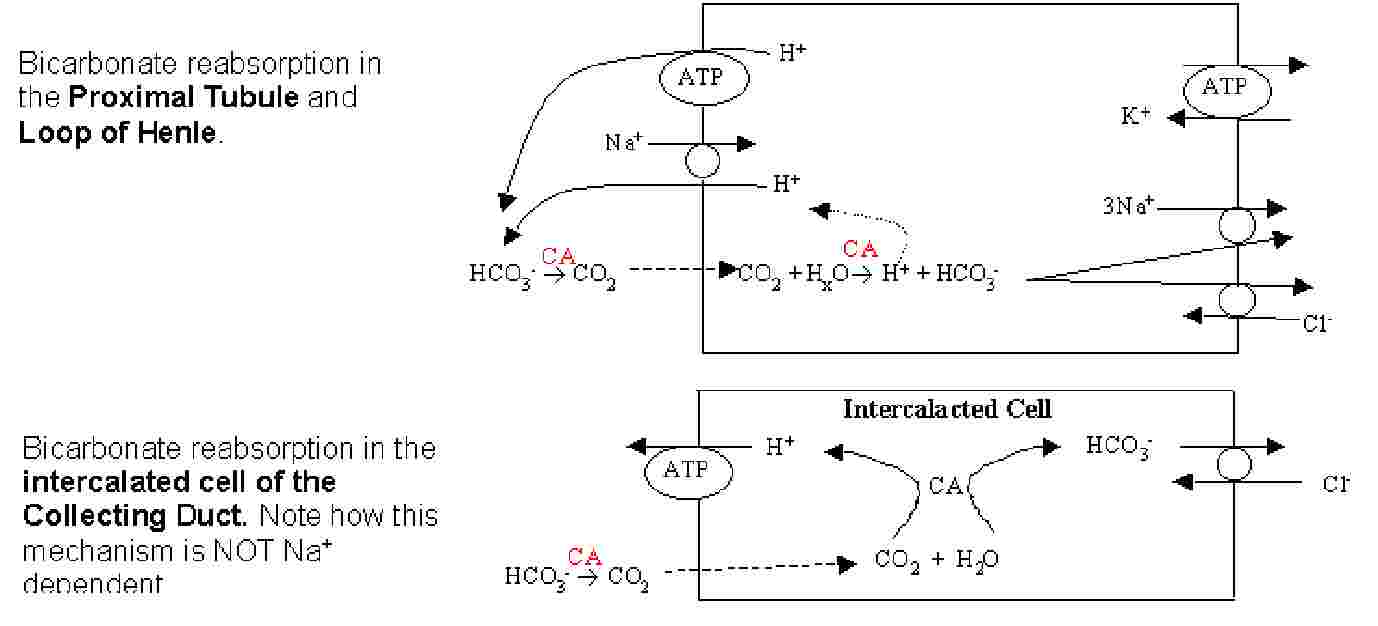
HCO3- Reabsorption in the Nephron
Regulation of HCO3- reabsorption
HCO3- reabsorption in the proximal tubule increases with an increase in filtered load and decreases when the filtered load is reduced. This happens because HCO3- reabsorption is coupled to Na+ reabsorption (Na+/H+ antiport). Recall that when ECV drops angiotensin II increases the activity of the Na+/H+ exchanger thus reabsorbing Na+.
Systemic acidosis stimulates HCO3- reabsorption in the whole nephron. This occurs because H+ secretion is favored, further upregulating the various H+ pumps (in the intercalated cells acidification results in the insertion of more H+-ATPases into the apical membrane). Systemic alkalosis has the opposite affect.
Aldosterone stimulates H+ secretion by the intercalated cells of the collecting duct. The mechanism for this is not yet known. (recall that aldosterone also has an affect on the principal cells of the collecting duct, it induces transcription of ENaC and Na/K ATPase).
Formation of new HCO3-
The reabsorption of HCO3- is important for the maintenance of acid-base balance. HCO3- loss in the urine is equivalent to the addition of H+ to the body. However, HCO3- reabsorption alone does not replenish the HCO3- that was lost during the titration of the non-volatile acids produced by metabolism. As such the kidney must replace the lost HCO3- with new HCO3-. To do this the kidney excretes H+ using two different buffers. HCO3- is produced in the cell from the hydration of CO2 and is added to the blood.
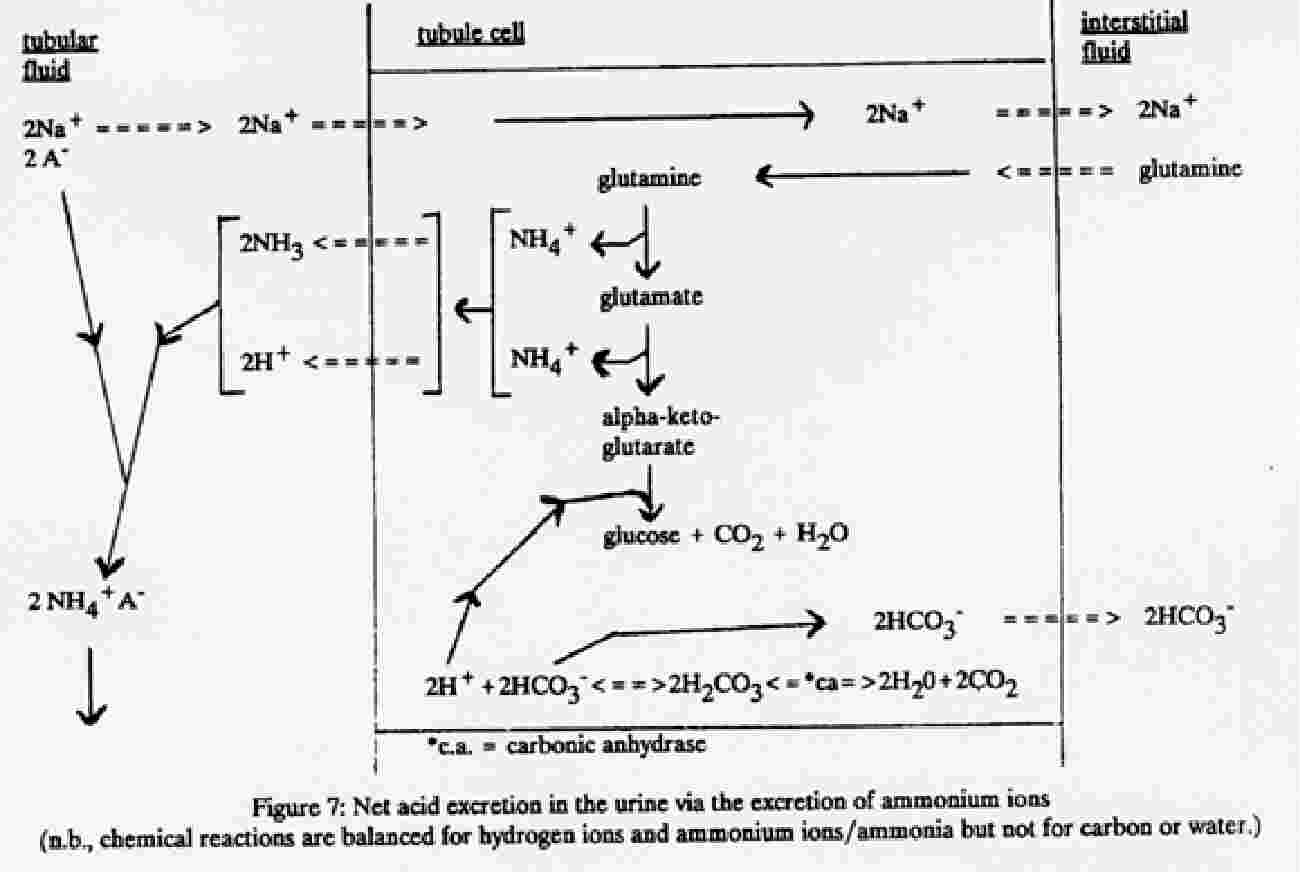
The two buffers used are: ammonia and phosphate. Phosphate is derived solely from the diet. Ammonia is produced by the kidneys, and is therefore more important than phosphate because its synthesis and excretion can be regulated in response to the acid-base requirements of the body. For example during systemic acidosis the enzymes in the proximal tubule responsible (see below) for the metabolism of glutamine are stimulated. This process takes several days for adaptation. As a result increased NH4+ production allows more H+ excretion and enhanced production of new HCO3-. Conversely, alkalosis reduces NH4+ production.
Production of NH4+ takes place in the proximal tubule, after which it is secreted into the lumen and then reabsorbed downstream by the thick ascending limb, in the interstitium it is converted into NH3 which then readily diffuses into the collecting duct where it is happily protonated to NH4+ by the acidic tubular fluid.