- Neonates: Staphlycoccus aureus (80%), Group B Streptococci, E.coli
- Children: Staphylococcus aureus, Group A Streptococci
- Adults: Adults with compromised health: Chronically debilitated patients (gram+rods), peripheral vascular insufficiency (polymicrobic or anaerobic), Diabetes mellitus, Sickle Cell Disease (Salmonella), Drug addicts (Pseudomonas, Staph)
- Direct innoculation of bone (open fracture, trauma, puncture wounds)
- Contiguous Spread (diabetic foot)
- Hematogenous seeding (blood borne) – most common – via bacteremia, systemic or distant extraosseous infection
- Neonates : Metaphysis and Epiphysis – metaphyseal vessels penetrate the growth plate communicating the two parts of the bone. Infection can cause destruction of the growth plate. Joint infection is most commonly seen at this age.
- Children : Metaphysis – metaphyseal vessels loop away from the growth plate forming capillary loops that act as dilated venous sinusoids. Capillary loops allow for areas of sluggish, turbulent blood flow which sets up the background for seeding of infection. Progression: Trauma Þ thrombus formation after trauma Þ bacteria collection Þ inflammatory response Þ damage to endothelial lining of blood vessels Þ necrosis.
- Adults : Metaphysis, epiphysis, subchondral bone – after growth plate closure, the metaphyseal vessels reunite with epiphysis exposing all areas of bone to infection
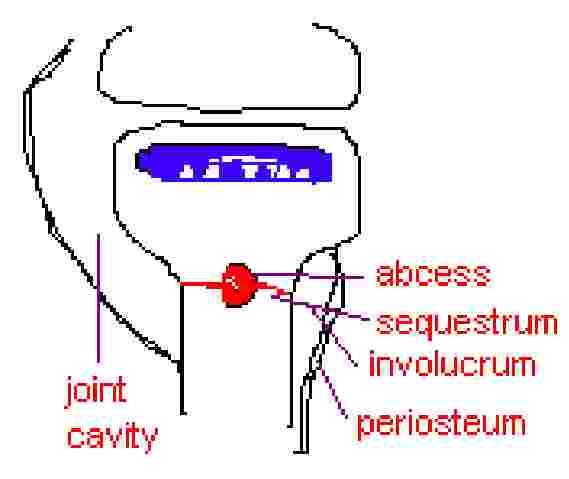
- Infection causes formation of SEQUESTRUM: necrotic bone resulting from destroyed blood vessels in the cortex that have thrombosed
- Increased intraosseous tissue pressure within abscess allows infection to penetrate Haversian system (Volkman’s canals)
- Infection spreads along paths of least resistance going horizontally to subperiosteum
- Periosteum reacts to infection by trying to replace necrotic bone with new bone (INVOLUCRUM: reactive viable bone) Þ periostieum elevates tearing the periosteal vessels causing thrombosis of these vessels and formation of more sequestrum (especially in neonates) – endosteum will also react
- Osteoclastic resorption of necrotic bone
- Appositional new bone formation (involucrum- similar to a cast of pus) and creeping substitution (new bone replacing necrotic bone)
- Dead vs. Necrotic bone: necrotic bone – no nuclei in lacunar spaces. This takes 2 to 4 wks to be seen. Osteoclasts may be seen resorbing bone with nuclei. This bone is "dead" bone – recognized by osteoclasts as necrotic bone (although microscopically not seen as necrotic because of present nuclei).
- REVIEW: Bacaterial proliferation Þ inflammatory response Þ Ý intraosseous pressure Þ ß blood flow Þ abcess formation Þ haversian spread Þ subperiostal destruction (periosteum elevation) Þ involucrum formation Þ sequestrum
- Histology : fibrin, granulation tissue
- Acute hematogenous
- Clinical Manifestations : pseudoparalysis, localized: tenderness, erythema, swelling, systemic: fever, malaise
- can act like cellulitis (early stages) or abcess (late stages)
- Treatment : antibiotics (broad spectrum, IV), surgery
- Clinical Manifestations : localized nagging pain
- Treatment : surgery, antibiotics
- usually due to inadequate treatment with antibiotics or inadequate surgical debridement of necrotic bone
- Histology : lymphocytes, fibrous cells (evidence of chronic inflammation)
- Treatment : surgical debridement, Antibiotics (6wks IV, 6more P.O.)
- Clinical Manifestations : multifocal, nonpyogenic, inflammatory osteomyelitis
- Treatment : NO treatment helps