medial side of knee has attachments (medial collateral ligament) whereas the lateral side does not due to the popliteus
makes knee vulnerable to a clip on the knee from the lateral side which will tear the components of the terrible triad
terrible triad = MCL, medial meniscus, ACL
medial meniscus = semicircle; lateral meniscus = almost complete circle (~340 degree loop)
between the menisci on anterior side = ACL; on posterior side = PCL; hint: cross 3rd digit over 2nd digit for orientation
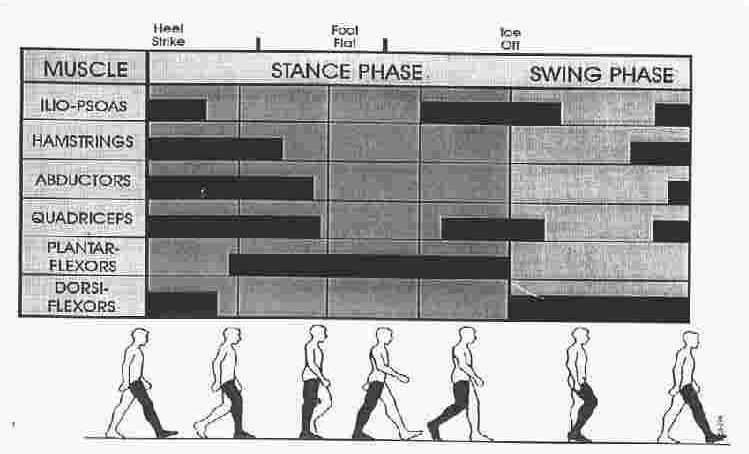
Mechanism of Gait
Bipedal gait is a learned activity; each person has an idiosyncratic gait. All other animals locomote like all of their species.
Gait cycle: from heal strike on one foot to heal strike on the same foot.
(1) Stance Phase
: when one is supporting themselves = heal strike (when heal hits the ground), foot strike (when heal of the foot is on the ground), toe off (when up on toe and about to kick off)
(2) Swing Phase
: when one’s leg is swinging = early swing, late swing
Walking is about getting one’s foot behind one’s center of gravity
for quadruped this is always true so anything that generates friction in rear direction causes forward motion
for biped we have to get our center of mass (pelvis in front of S2) out in front of our feet, which is inefficient.
this requires that we balance over our hip because it is a frictionless ball-n-socket joint.
Plumb line from Center of mass would run in front of knees and ankles but slightly behind hip
So we should pitch back on hips and buckle forward in the knees and ankles looking like a concertina
Ileofemoral ligament (large) [from AIIS to inner trochanteric line on femur] stops us from pitching back
Knees don’t buckle in the wrong direction because of the anterior cruciates and collateral ligaments
Ankle has no ligament due to need for motion there; when rocking forward, center of mass goes in front of the feet, so plantar flexors are fired to push us back. This is how we stand.
Walking bipedally is done one leg at a time. We are the only animal that can stand on one leg because the abductors: Gluteus Medius, Minimus and Tensor fascilata contract with every step we take and hold us up.
The reason that women have much greater failure of joints is that they have wider hips due to the birth canal. Note that the wider the hip the greater the horizontal component of the quad-vector, which works in opposition to the fibers of fascia medialis (which fire late in extension cycle to hold the patella in place). This leads to
Ý Ý stress on knee
In the hip, the abductors run from the greater trochanter to the pelvis. The center of rotation is in the middle of the femoral head which acts as a fulcrum between the center of mass and the force of abductors. A wider hip extends the moment arm between the center of mass and the fulcrum of the female pelvis. Therefore greater abductor force is required to balance to same mass thus increasing the joint reaction force considerably.
Muscles of Gait cycle
Acceleration of thigh is the action of the Iliopsoas and Rectus femoris. Rectus femoris is important because sprinters can tear this off the anterior inferior spine where it originates- comes off easily due to cartilaginous apophysis attachment.
Deceleration
is accomplished by hamstrings which come across the hip joint and contract eccentrically (elongating).
So hamstrings are pulled by athletes who decelerate quickly or kick
Þ pulling the muscle off the ischial tuberosity.
Heal Strike
fires the Dorsiflexors (anterior tibial group:Tibialis anterior etc., deep fibular n. ) eccentrically contract and lower the foot to the ground. Quadriceps eccentrically contract to absorb energy as knee goes into 5o flexion; this prevents the knee from buckling
Foot Strike
: abductors contract to hold body up. As center of mass moves forward the Plantar flexors (triceps surae: gastrocnemius, soleus, and plantaris) contract to push body ahead.
Toe off
: Quadriceps concentrically contract to help the plantar-flexors push body ahead by elongating lower limb.
Muscle Knock-out Effect on Gait
Abductors
(glutei minimus, medius, tensor fasciae latae): loss due to injury to superior gluteal nerve, makes it impossible to stand on one leg because the unsupported side of leg will collapse = Positive Trendelenburg Sign. So to compensate one must lean over the hip on the side off the bad leg. This is called Trendelenburg or Gluteus Medius Gait.
Quadriceps
: this is the only extensor of the knee, so when going into heal strike the knee will buckle. The only way to walk is to lean forward and force the leg into extension by holding the knees in place with one's hands.
Iliopsoas
: if this is lost, then Rectus can be used. If both groups are lost, then there are no muscles to flex the thigh and accelerate the limb. The compensatory gait uses the momentum of one’s body to swing the limb around from the hip.
Plantar-flexors:
the only other muscle group that makes the lower limb long is the Quads, which can be used to compensate for a deficit in the Plantar-flexors. If the knee can be bent, the quads can be used to extend the knee.
Dorsi-flexors:
most common problem because the common fibular nerve runs around the fibular head and is at risk for being cut if knee is clipped to point of breaking fibular head which can cut into nerve. This takes out dorsi-flexors which prevents picking up the toe during swing phase. High stepping gait compensates so results in clopping