When quantifying the effects of a drug a separate dose-response curve is required for each effect of the drug in question.
What are the dose-response curves that can be used?
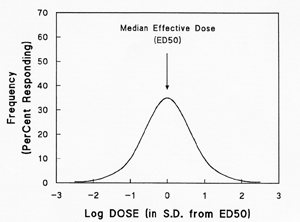
Log-dose response curves (LDR):
(1) Quantal curves
– describing a population.
(a) Frequency distribution curve: shows that in any given population, a range of doses is necessary to achieve a single, given effect in each of the individuals of that population. The dose at which 50% of the individuals show the response has been arbitrarily set to zero. Note the numbers at the x-axis are not true values, but standard deviations from the mean corresponding to ED50. Standard deviations are just a way to express about how far away a value is from the mean, so 68% of the values are always 1 s.d. away, and 95% are 2 s.d. away. Example: in the graph, 35% of the population was affected at a Log dose 0, while only 10% needed a higher Log dose 1 to be affected.
(b) Quantal log dose-response curve: The LDR is a simple way to determine the ED50 (the effective dose, 50%). The ED50 for an LDR is the drug dose at which 50% of individuals will have responded. The LDR also allows an estimation of the concentration of drug required to produce a response in the entire population. Example: in graph, at least 85% of population was affected after a Log dose 1, and almost everyone was affected after a Log dose of 2.
(2) Graded curves
– describing an individual subject.
(a) Graded log dose-response relationship: shows intensity of response (the effect) in an individual subject versus dose. The plot looks the same as that for the quantal curve. It can be viewed as having the following characteristics:
(b) Potency – size of pill, or the dose of drug required to produce a given effect. It is of little importance pharmacologically. Only useful to determining the ED50 of a drug.
(c) Efficacy – maximal effect produced by a drug. Efficacy is of great importance clinically, more important than potency.
(d) Slope – steepness at which the effect changes as a function of dose. This can vary dramatically between agents. It is of importance in adjusting dosage in a patient and in safety of administration; range over which all of you are going to respond
(e) Variation – all patients will respond differently.
How do we evaluate the usefulness of a drug?
A drug can have: therapeutic effects, side effects, or toxic effects
ex: phenytoin/dilantin – 1st order becomes 0th order – anticonvulsent for epilepsy – side effects (during puberty) include hirsutism (increased facial hair) and gingival hyperplasia – not bad for boys, unacceptable for girls
ex: propranolol – beta adrenergic antagonist,
ß ventricular contractility (good for MI), ß renin release (lowers angiotensin and blood pressure), ß refractory period at AV node (side effect – not therapeutically significant)
if you have a superventricular arrhythmia, what was a side effect is now a therapeutic effect
Whether the therapeutic effects of a drug are desirable or not is an arbitrary decision. As such, side effects may in some situations be considered desirable.
Toxicity:
(1) extension of the therapeutic effect which occurs on the same dose response curve at a higher [drug] (ex: giving too much anticoagulants can cause bleeding)
(2) side effect unrelated to the therapeutic effect. Therefore has its own dose response curve (ex: too much morphine for pain will cause respiratory distress).
In the graph to the right can see that at a high enough dose the drug can have toxic effects.
At a high enough toxic dose the drug becomes lethal.
benzodiazapines are safe; chloral mydlcate is dangerous – if you want 75% sedated, will kill 10% of people
TD50 = toxic dose, 50%
LD50 = lethal dose, 50%
THERAPEUTIC INDEX
or THERAPEUTIC RATIO = TD50 / ED50
you want this ratio to be as big as possible, indicating you’d have to give a lot of drug in order to achieve toxicity. i.e. shift right on the x-axis
Þ changes with time and person or population; different effects; don’t expect 100% of people to respond.
Drug-Receptor Interactions
In pharmacology a receptor is anything that binds something else. Ex: hemoglobin is an O2 receptor. Ex: DNA binds stuff.
Assumptions:
(1) drugs interact with receptors in accordance with the Law of Mass Action (see next page).
(2) Each receptor has a single binding site for a drug, though it can bind different classes of drugs at same site.
(3) [drug] >> [receptor]
(4) occupancy assumption: response to drug
a receptor occupancy by drug
Law of Mass Action: Drug + Receptor
Þ Drug-Receptor Þ Effect
Effect = (Effectmax x [Drug]) / (KD + [Drug]) or Effect / Effectmax = [D] / ([D] +KD)
equation is similar to Michaelis-Menton
note: plotting Effect/Effectmax vs log [drug] yields the graded LDR and the KD is analogous to the ED50 of the graded LDR.
Agonist
– a drug which activates (stimulates) a receptor and its associated "effector system" to perform its action or effect
has greater affinity for the active form of the receptor
Antagonist
– a drug which prevents or blocks a receptor and its "effector system" from initiating and performing its action or effect. An antagonist will have no observable effect in the absence of its agonist.
Two types of Antagonism
:
(1) Competitive Antagonism – can be overcome by increasing the [agonist]. Reduces the apparent affinity (ED50) of the agonist for the receptor. (mnemonic: the curves chase each other in competitive antagonism).
(2) Non-Competitive Antagonism – can not be overcome by increasing the [agonist]. Reduces the maximal effect (Emax) but does not alter the apparent affinity (KD or ED50).
has greater affinity for the inactive form of the receptor
Partial Agonist
– a drug having both agonist and antagonist properties. In reality it appears like a weak antagonist in the presence of an agonist. Increasing concentrations (dose) of a partial agonist (via its antagonist property) will reduce the response to the full agonist only to a level equal to that produced by maximal doses of the partial agonist alone (via its agonist property).
has Ý affinity and ß effect compared to full agonist
Inverse Agonist
a drug which shifts the receptor from active to inactive state.
Note: many receptors have some portion of their population in an active conformation, even in the absence of the receptor ligand.
Receptors
Subtyping
Rank Order of Potency
– receptors are classified by functional criteria. This means that in the laboratory they are exposed to a range of substrates for each of which a dose-response curve is drawn. These results are then compared and the receptors are functionally classified by potency.
ex: a (norepi) and b (epi)Þ 2 patterns seen through body, therefore thought 2 different receptors with 2 different pathways
b
Þ INE > epi > norepi > dopamine > PE - muscarinic and nicotinic
a
Þ norepi > epi > PE > dopamine >> INE - much more expansive
Receptor Regulation
– Maguire’s Law of Receptors:
Ability of receptor to respond is inversely proportional to the history of stimulation
Ý
stimulation, ß response
This means that the more you stimulate a receptor the less response you’re gonna get, and vice-versa.
[R] can change: chronic stimulation = ß [R], no stimulation = Ý [R]
Drug actions not mediated by Receptors
Interaction of drugs with small molecules
: Ca-EDTA as chelating agent antidote for heavy metal poisoning.
Nonspecitifc effects
: Osmotic diuretics (increase osmolarity of tubular urine leading to slow water reabsorption and diuresis), Antacids (neutralize excess acid in stomach), detergents, disinfectants, anesthetics (membrane depressants).
Incorporation of a drug into a macromolecule
: drug replaces normal metabolite and is falsely incorporated into a normal product. The now defective product produces the effect.