can also use thin lines (thick lines bolded): 300, 250, 214, 187, 167; 150, 136, 125, 115, 107; 100, 94, 88, 83, 79; 75, 71, 68, 65, 62; 60
(2) if bradycardic (less than 60 bpm) or irregular: count 6 second strip (2 3-second marks) and multiply by 10
can also count entire strip (10 seconds) and multiply by 6
(3) calculate: 1500/number of small lines between similar waves
must determine coexisting independent rates if there are more than one
Rhythm
Automaticity
– heart has automaticity foci that respond at different rates and produce different morphology on EKG
atrial – preceeded by P wave (shape of P wave changes depending upon originating focus), narrow complex QRS, normal rate 60-80/min
junctional – no P wave, narrow QRS, normal rate 40-60/min
ventricular – no P wave, wide QRS, normal rate 20-40/min
Intervals
PR should be less than 0.2 seconds (one large square)
QRS should be less than 0.12 seconds (three small squares)
QT interval – must be corrected for rate (QTc); in general, QT should be less than half R-R interval
Sinus Rhythm
– P before each QRS, QRS after each P, P in correct orientation (up in II)
normal sinus rate is 60-100 bpm; if sinus rhythm but greater than 100 bpm, it is sinus tachycardia; if less than 60 bpm, it is sinus bradycardia
Irregular Rhythms
Sinus Arrythmia – varies with respiration, P waves identical; not pathological
Wandering Pacemaker
– irregular rhythm, P waves change shape, rate less than 100 bpm
Multifocal Atrial Tachycardia
– same as wandering pacemaker with rate greater than 100 bpm
Atrial Fibrillation
– irregular ventricular rhythm without P waves; may see erratic atrial spikes or wavy baseline
Escape
– lower level of heart will automatically respond if not driven with faster rate from above (automaticity)
Escape Beat
– single beat after a pause; can be atrial, junctional, or ventricular
ventricular escape beats can be caused by burst of excessive parasympathetic activity (parasympathetic innervation inhibits SA node and AV junction but NOT ventricular tissue)
Escape Rhythms
– persistent escape beats (sinus node not active or not conducting); can be atrial, junctional ("idiojunctional" rhythm), or ventricular ("idioventricular" rhythm)
idiojunctional rhythms can produce retrograde atrial depolarization with an inverted P' before, during, or after the QRS
idioventricular rhythms caused by complete block below AV junction (P waves present but not associated with QRS) or total failure of all tissue above ventricles (downward displacement of the pacemaker)
idioventricular rhythms can cause loss of consciousness due to insufficient cardiac output (Stokes-Adams Syndrome)
Premature Beats
– from an irritable automaticity focus; can be atrial (PAB), junctional (PJB), or ventricular (PVC; 6 PVC's per minute is pathological)
PAB/PJB – irritable atrial and junctional foci are caused by sympathetic stimulation, caffeine, amphetamines, cocaine, digitalis, toxins, ethanol, hyperthyroidism, and stretch receptors
PAB resets from the new P' wave at previous rate (first cycle slightly lengthened due to transient baroreceptor reflex)
PAB's can cause wide QRS (aberrent ventricular conduction)
PAB and PJB still depolarize the SA node (either directly or through retrograde atrial depolarization) and reset the pacing, so rhythm begins again in phase with the premature beat
if the beat is not conducted (due to refractoriness), the missed QRS in produces a long empty baseline (harmless)
can occur every other beat (atrial or junctional bigeminy) or every third beat (atrial or junctional trigeminy)
PVC – irritable ventricular foci are caused by low oxygen, hypokalemia, or muscle pathology (mitral valve prolapse, myocarditis, etc.)
PVC's do not depolarize the SA node, so there is a "compensatory" pause after them (except for "interpolated" PVC's, where they occur exactly where the ventricular contraction would have)
P waves continue unaffected and the next QRS occurs where it would have if there had been no PVC
a PVC that falls on a T wave ("R on T phenomenon") can cause sustained ventricular tachycardia
ventricular parasystole
– ventricular tissue with entrance block (NOT an irritable focus) that starts PVC's at its own automatic firing rate
Tachyarrhythmias
Paroxysmal tachycardia
– 150-250 bpm; can be atrial (PAT), junctional (PJT), or ventricular (PVT)
atrial (PAT) or junctional (PJT) are also called paroxysmal superventricular tachycardia (PSVT)
paroxysmal atrial tachycardia with block (PAT with more than one P wave before each QRS) – caused by digitalis
AV nodal reentry tachycardia (AVNRT)
is a type of PJT
PJT may still have retrograde atrial depolarization and inverted P' waves
PJT may involve somewhat widened QRS since one bundle branch may still be refractory when next beat arrives (aberrent ventricular conduction)
PVT:
during PVT, if the P wave appears at just the right time, can see normal QRS (capture beat) or QRS that degenerates into a PVC (fusion beat)
PVT can be distinguished from PSVT with wide QRS (caused by BBB, etc.) by the following:
presence of coronary artery disease
very wide QRS (more than 0.14 sec)
extreme RAD
AV dissociation (see capture or fusion beats)
Torsades des Pointes
– "party streamer"; caused by two competitive, irritable foci in different ventricular areas
Flutter
– 250-350 bpm; can be atrial (sawtooth baseline with QRS's) or ventricular (sine wave; almost always leads to fibrillation unless treated)
Fibrillation
– greater than 350 bpm; can be atrial (jagged baseline with QRS's) or ventricular (no identifiable waves)
no pumping occurs
atrial fibrillation can produce a narrow-complex tachycardia (rapid ventricular response)
– spontaneous pause in electrical activity; can restart automatically or have an escape beat (see above)
AV Block
– causes abnormal PR interval
1st degree block
– PR too long (greater than 0.2 seconds, or one large square)
2nd degree block
– some P waves without QRS:
Wenkebach (Mobitz I)
– block at the node itself; PR gradually lengthens until a P does not produce a QRS
Mobitz II
– block beyond the node; PR length constant, but some P waves do not produce QRS (can be 2:1, 3:1, etc., or even intermittent)
2:1 block can be either of above; can use vagal maneuvers to differentiate (see below)
3rd degree block
– none of the P waves get through; there is an idioventricular or idiojunctional rate instead
Bundle Brach Block
– basically two out of phase QRS's (R R'); requires wide QRS for diagnosis (at least 3 small squares; best to use limb leads since low voltages allow for more accurate measurement)
Right Bundle Branch Block (RBBB)
– QRS has two peaks (R R') in V1 or V2 usually returning to lower than baseline between them
Left Bundle Branch Block (LBBB)
– QRS has two peaks (R R') in V5 or V6 with slight depression between them
BBB makes ventricular hypertrophy criteria unreliable
LBBB makes infarction difficult to determine
BBB can cause SVT to degenerate more easily into VT
Hemiblock
– block of anterior or posterior fascicle of LBB; causes axis deviation and widened QRS
Anterior hemiblock
– left axis deviation with a Q wave in I and a prominent S wave in III
Posterior hemiblock
– right axis deviation with a prominent S wave in I and a Q wave in III
can have bifascicular blocks (RBBB + hemiblock)
must have previous EKG to diagnose so that other causes of axis deviation can be ruled out
Vagal Maneuvers
(gagging or carotid sinus massage) – inhibit irritable atrial or junctional foci or increase the refractoriness of the AV node
abolishes PSVT, identifies 2:1 AV block (no effect if Mobitz II), and reveals flutter waves in atrial flutter
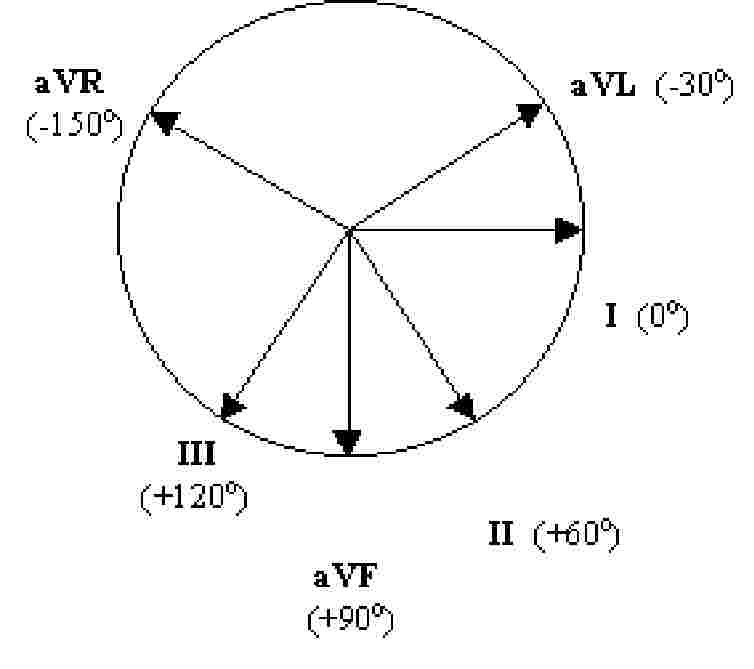
Axis
find axis quadrant using below diagram (QRS above or below baseline in each lead):
axis is also 90 degrees from isoelectric QRS (same up as down) or in the direction of a QRS that only goes up (opposite direction of QRS that only goes down)
Normal axis is "up in I and aVF" (some say "up in I and II")
if I is down: right axis deviation (RAD)
if aVF is down: left axis deviation (LAD)
if both are down: extreme RAD
Axis Rotation – find isoelectric QRS (same up as down) in chest leads (V1 to V6); normally occurs in V3 or V4
if isoelectric in V1 or V2: rightward rotation
if isoelectric in V5 or V6: leftward rotation
Hypertrophy
Atrial Hypertrophy
– diphasic P wave in V1
right atrial hypertrophy
– large initial component of diphasic P wave in V1
left atrial hypertrophy
– large terminal component of diphasic P wave in V1
Ventricular Hypertrophy
– tall R wave in V1 for RVH, deep S wave in V1 and tall R wave in V5 for LVH
right ventricular hypertrophy
– widened QRS with RAD, rightward rotation, and:
R greater than S in V1 but R gets smaller in V2 through V6
S wave persists in V5 and V6
left ventricular hypertrophy
– widened QRS with LAD, leftward rotation, and:
sum of depth of S in V1 and height of R in V5 is more than 35 small squares
inverted T wave with gradual downslope and rapid upslope
Infarction
– always requires previous EKG for comparison
Identifying Injury
(1) ischemia
– inverted T waves (earliest sign) – symmetrical down- and upslope, opposite direction of QRS
(2) acute injury
– ST elevation
can occur without Q waves: "non Q-wave MI"
ST depression may indicate "subendocardial infarction" (small shallow area as opposed to entire wall of heart)
(3) necrosis (non-conductive tissue)
– Q-waves
significant if more than one small square wide or greater than 1/3 the amplitude of the QRS
remain even after acute infarction is over (unlike other two)
Localizing Injury
– leads where the above occur; also remember that axis points away from infarction
Anterior
– left anterior descending artery – V1 to V4
Lateral
– circumflex artery – I, aVL
Inferior
– right or left coronary artery – II, III, aVF
Posterior
– right coronary artery – V1 and V2, but changes are mirror image (R instead of Q, ST depression instead of elevation, etc.)
for blocks and hemiblocks: AV node is supplied by the right coronary artery, RBB and anterior LBB is supplied by LAD, posterior LBB is supplied by either
Effects of Other Medical Conditions on EKG
Pulmonary Embolism
prominent S wave in I
Q wave in III
inverted T waves in III and V1 through V4
ST depression in II
acute incomplete RBBB
RAD with rightward rotation
Electrolyte Disturbances
hyperkalemia
wide flat P – P disappears entirely with severe hyperkalemia
wide QRS
peaked T wave
hypokalemia
flat T wave
U wave (after T wave; represents Purkinje cell repolarization) – prominent with severe hypokalemia
can cause torsades des pointes if extreme
hypercalcemia
– shortened QT interval
hypocalcemia
– prolonged QT interval
Drugs
Digitalis
therapeutic – ST slopes below baseline, inverted T waves, shortened QT
excessive – blocks: SA block, paroxysmal atrial tachycardia (PAT) with block, AV block (can be 3rd degree)